
Near-patient Bilirubin Testing to enable Neonatal Care at Home Challenge

As part of the Women's & Children's Health Innovation Portfolio, the Scottish Government Chief Scientist Office (CSO), the Scottish Government Directorate for Children and Families and the Royal Hospital for Children, Glasgow and Glasgow Children's Hospital Charity are funding this Small Business Research Initiative. The West of Scotland Innovation Hub are hosting this challenge on behalf of NHS Scotland.
Near-patient Bilirubin Testing to enable Neonatal Care at Home Challenge
As part of the Women's & Children's Health Innovation Portfolio, the Scottish Government Chief Scientist Office (CSO), the Scottish Government Directorate for Children and Families and the Royal Hospital for Children, Glasgow and Glasgow Children's Hospital Charity are funding this Small Business Research Initiative. The West of Scotland Innovation Hub are hosting this challenge on behalf of NHS Scotland.
The open innovation challenge provides an opportunity for organisations, working in partnership with regional Innovation Hubs to develop disruptive innovative solutions that focus on the monitoring of jaundiced newborns at home. These solutions will focus on near-patient bilirubin testing to develop innovative care pathways and enable family centred care at home for babies who do not require to be in hospital.
The challenge is now open for applications from the Public Contract Scotland website until 13th December 2023
Applicants can apply for a share of £220,000, inclusive of VAT over a 2-phase competition. Phase 1 is allocated £60,000 for up to 4 projects. Phase 1 projects can range in size up to total costs of £15,000 inclusive of VAT. Phase 2 is allocated £160,000 for up to 2 contracts. Phase 2 projects can range in size up total costs of £80,000 inclusive of VAT.
A briefing event to provide further background and an opportunity for applicants to ask questions will take place on 25 October at 10.00 am. Please register here
All questions should be directed to the Q&A portal on PCS before 11am UK time on 6th December 2023 or at the Q&A session during the briefing event.
Challenge Objective
Innovative solutions are sought for near-patient bilirubin monitoring of newborns which are accurate, efficient, safe, accessible and equitable. These solutions will enable the development of innovative care pathways.
Solutions must be working towards compliance with UKAS accredited point of care testing (POCT) (ISO15189:2022) methodology for analysis.
When fully developed, solutions must include a real-time process to incorporate results into NHS Scotland electronic patient records.
The solutions will have the potential to revolutionise care at home for both babies and healthcare services globally. The commercial potential across growing UK and global neonatal markets is 140 million births per year (£8billion market size ).
Background
Existing models of neonatal care
The care of babies in neonatal units and maternity hospitals ranges from extremely premature babies needing complex care, to the larger number of babies that could be cared for at home but remain in hospital, separated from their parents, as the care they require is currently only available within a hospital. Examples of this are treatment for jaundice, types of feeding and treatment to keep babies warm and monitor weight. This separation of otherwise well babies who could be at home has an enormous impact on families and bonding, in addition to reducing the availability of scarce cots within Neonatal units, beds within maternity hospitals and avoidable costs to the NHS. This challenge affects babies and parents in every maternity hospital, the scalability and hence impact of solutions will be significant.
Jaundice: a common neonatal problem
Jaundice is an almost universal phenomenon in the newborn, affecting 60% of term babies in the first week of life . In the UK in 2021 660,000 live births were registered. Jaundice is caused by raised levels of bilirubin (hyperbilirubinaemia), leading to yellow discoloration of the skin and sclera.
It is generally benign and transient, but if it is severe and untreated may lead to permanent behavioural and neurological impairments.
Phototherapy in hospital is the mainstay of treatment of jaundice, and is effective at preventing these complications. A typical course of phototherapy lasts 2-3 days. The impact of separation from siblings, fathers and other family members at this unique time for bonding is substantial.
Approximately 6% of all admissions of term babies to UK neonatal units are for jaundice therapy . Our data suggest that many of these patients could be treated at home.
During a two-month monitoring period across NHS Greater Glasgow & Clyde Health Board in 2022, 77 babies required inpatient admission to a neonatal unit for phototherapy treatment for uncomplicated jaundice. The phototherapy course for these babies accounted for 178 additional maternal bed days (in the two month period) for mothers and babies who did not require any additional specialised in hospital care. Extrapolating this data, in NHS Greater Glasgow and Clyde alone it is equivalent to ~900 maternal bed days per annum and a cost approaching £1 million pounds
A survey of 29 parents and carers over the same two-month period found that 90% would have preferred phototherapy treatment at home.
To achieve these important potential benefits of home phototherapy, a first essential component of the care pathway is accurate, rapid jaundice testing in the home environment.
Developing home-based jaundice care
An effective and efficient home phototherapy service complements the strategic aims and objectives of NHS Scotland and aligns with the individualised patient-centred approach that underpins “The Best Start”, a 5-year plan for Maternity and Neonatal Services across NHS Scotland, prioritising family centred care and care at home.
Home phototherapy is effective – phototherapy is a proven treatment for jaundice, and evidence shows that standard practice can be successfully adapted to the home environment. Home phototherapy is person-centred – respecting the importance of family bonding in the early newborn period and promoting shared decision-making. Home phototherapy is safe – the burden of avoidable harm does not increase significantly as long as parents and carers have appropriate access to advice and support.
Home phototherapy represents a significant addition to the spectrum of care currently delivered – reducing bed days while improving patient satisfaction. To quote one of our parents, “I truly believe that there should be funding made available for something like this!”
Challenges of current jaundice testing in new-born
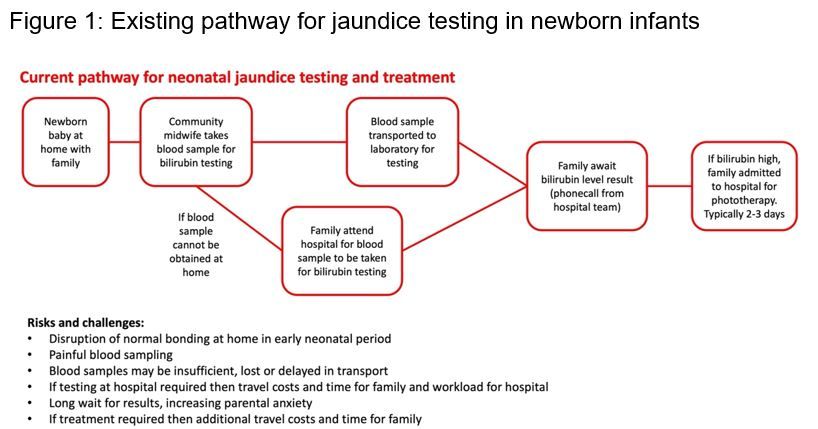
However, for jaundiced babies both in hospital and at home the challenging aspect of their patient journey is testing and monitoring of jaundice or ‘bilirubin’ levels. At present a blood test is required (approximately 0.25mls blood), which is then transported to the laboratory and then analysed, Figure 1. There are several problems with this current system – it can take several hours, there can be insufficient sample volume, samples can be mislabelled and samples can be haemolysed meaning there is no result and the blood test has to be repeated which is distressing to families and delays clinical treatment decisions. The current system also depends on several staff members – the individual taking the sample, personnel involved in transporting the sample, the laboratory staff and then the individual who is responsible for looking out for the result and deciding if any treatment is required then communicating this treatment plan. The current system is not efficient or patient centred, with errors and challenges identified at each point of the process map and we are looking for innovative ways to improve and streamline this system.
The project team hosted a stakeholder event in March 2023 which was attended by members of the multidisciplinary team caring for jaundiced babies and have held several meetings with other Health Boards across Scotland. They unanimously agreed that innovative solutions for near-patient or point of care patient bilirubin monitoring would be most welcome and an aspect of care that has the opportunity to improve the efficiency of patient care and has scalability to every maternity service in the UK.
Progressing near-patient testing of bilirubin in the home environment for babies requiring treatment for jaundice, would also address existing care inequalities and impact on sustainability and the environment by reducing parent and staff travel. Sustainability and reducing inequalities are key strategic priorities of NHS Scotland.
We would like to focus this challenge on an area that has potential solutions already in development, so we are interested to know if the market has solutions that address testing and recording for jaundice at home and/or out with the hospital setting.
Potential solutions would require to demonstrate an effective user friendly testing system, validation of the sample volume, quality and analytical performance, and must be working towards compliance with UKAS accredited point of care testing (POCT) (ISO15189:2022) methodology for analysis. When fully developed, solutions must include a real-time process to incorporate results into NHS Scotland electronic patient records.
Long term vision
The goal of innovation and service redesign is to deliver family centred care at home for babies who do not require to be in hospital.
Developing care at home is a current priority across all UK NHS services and within the maternity landscape offers an enormous opportunity to reduce unnecessary maternal bed and cot occupancy. It will undoubtedly improve patient flow through neonatal and maternity services.
In NHS Scotland with the move to centralisation of Perinatal care for the sickest mothers and babies, developing processes to minimise unnecessary maternal bed and cot occupancy supports this model. Ensuring the smallest and sickest patients can be treated in the right centre at the right time.
Near-patient bilirubin testing to enable neonatal care at home would:
• Achieve substantial cost efficiencies to the NHS by minimising unnecessary maternity and cot day’s usage.
• Improve maternal and family bonding in the newborn period by keeping families together, appreciating the positive long term impact this has on maternal and infant mental health.
• Impact positively on breast feeding rates with all the benefits for long term health and wellbeing this realises.
• Reduce waiting times for decisions on treatment of jaundice in the new born, impacting on the potential complications of untreated high bilirubin levels.
• Improve the patient journey and family experience of those experiencing neonatal jaundice. • Reduce health inequalities by widening this care pathway to families in more diverse geographical areas, a key ambition of NHS Scotland.
• Reduce staff and family travel impacting positively on sustainability and the environment.
• Support the long-term vision that neonatal care at home is embedded into normal clinical practice. Technology, patient monitoring systems and pathways with integration with the NHS patient record will all be in daily clinical use to realise this ambition. Patient satisfaction will increase, staff satisfaction will increase and efficiency of in patient resources will be optimised ensuring fiscal efficiencies to the NHS.
• Validate near-patient testing technologies with transferable potential to other adult and paediatric disease settings.